
Improve your implant planning for more predictable results
Dec 14, 2017
by Nicole Winitsky, DDS, PhDs, Specialist in prosthodontics
In my daily practice as a prosthodontist I treat young adults between 18-25 years, with implants. There is not much available in the literature about implants for young adults and the little that exists is mostly about infra position of the implant crown or case reports. Instead, I want to share some thoughts and highlights around the actual treatment procedure. Aside from a small amount of available literature, there are not really any other sites or forums either – at least which I know of – with information and discussions about this specific topic. There are only a few Q&A’s about it online, and the answers are quite old.
So what I am sharing here is based upon my own thoughts and my own experience, and it does not mean that I “invented” it in the first place. I however really try hard to create this type of clinical environment on a daily basis, and I am passionate about achieving this. Please do not hesitate to get in touch with me or share your comments below!
Missing teeth in young dentitions are generally caused by congenital absence of tooth germs (aplasia) or by trauma and are mostly located to the anterior maxilla. Most of the patients, missing one or maybe two teeth, are treated with single implants but there are also patients with larger traumas or multiple aplasias that needs implant bridges. The implant sites in patients suffering from aplasia or trauma often have very restricted bone volume and many of these young patients have high smile lines showing the whole implant crown including the papillas and soft tissues (fig 1). In contrast to implant treatment in adults the challenge with young patients is also that the treatment is expected to last for a very long time, in most cases at least 60 years. During these years continued growth and changes in the face occurs which causes the positioning of the implant crown to change over time1-4. Due to all of the above mentioned, these cases need to be planned and performed as optimal as possible both when it comes to implant placement, implant stability, emergence profile and shape and shade of the crown5.

Fig 1. 19-year old patient with high smileline prior to implant placement.
To plan for optimal implant placement
In earlier decades when implant treatment was less explored the dentist and the patient were satisfied with the implants being osseointegrated to enable loading with a prosthetic reconstruction. Today we know that patients, in need of especially frontal implants, not only wants a new tooth to chew with but also a natural looking tooth in a good positon. I also always strive towards making a screw retained reconstruction. In order to reach an optimal result both esthetically, functionally and hygienic we need to have a good multidisciplinary teamwork between dental technician, surgeon and prosthodontist. Today we have good tools for communication between these disciplines. We have digital planning programs for implant placement (fig 2) and we also have less sophisticated but still very good simple acrylic guides (fig 3). Today we talk about prosthetically driven implant treatments or “crown down” planning of our implant treatments. This means that the planning needs to start from where we want the implant crown to end up and according to that we plan the placement of the implant in the bone. Sometimes we have enough bone volume and sometimes the patient needs to go through bone augmentation procedures to increase our possibilities to place the implant crown in the correct position.
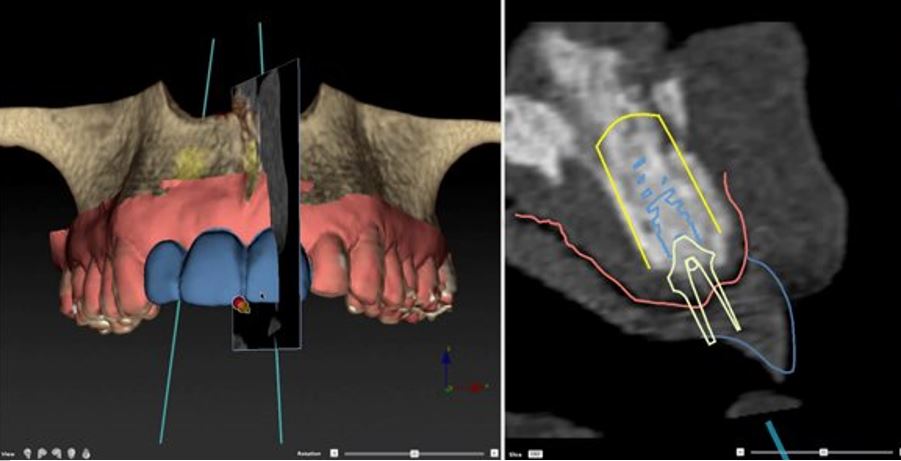
Fig 2. Planning of implant placement in digital program

Fig 3. Simple acrylic guide used for optimal implant placement
With this short text I would like to encourage more dentists working with dental implants to work with a more predictable treatment protocol by communicating with your implant team (dental technician, prosthodontist and surgeon) through using surgical guides. It starts with the dental technician waxing up where the future crown is supposed to end up. By showing the planned position of the crown to the surgeon with the help of a surgical guide and by using the guide at the placement of the implant the treatment becomes predictable. Both for the implant team and the patient. We thereby make our work both easier, more pleasurable and we will reach better treatment results (fig 4). All for the benefit of the patient. This might sound obvious but out in the clinic many cases are being treated without the different dental professionals understanding how they should work together to get a good end result. The key is to find an effective work flow including surgical guides that can be viable to many implant teams and patients all over the world.
A well planned and performed case is of course very important in all implant cases but maybe it is of extra importance that the treatments with anterior implants in young patients are well planned and performed due to the great amount of challenges to consider (mentioned above) specifically in these cases. Or how would you like your son or daughter to be treated?

Fig 4. Result of 19-year old patient with aplasias 12, 22. Result with screw retained zirconia crowns through successful collaboration. Simple surgical guide was used.
References:
- Jemt T, Ahlberg G, Henriksson K, Bondevik O. Changes of anterior clinical crown height in patients provided with single-implant restorations after more than 15 years of follow-up. Int J Prosthodont. 2006; 19:455-461.
- Thilander B, Odman J, Grondahl K, Friberg B. Osseointegrated implants in adolescents. An alternative in replacing missing teeth? Eur J Orthod. 1994; 16:84-95.
- Thilander B, Odman J, Jemt T. Single implants in the upper incisor region and their relationship to the adjacent teeth. An 8-year follow-up study. Clin Oral Implants Res. 1999; 10:346-355.
- Oesterle LJ, Cronin RJ, Jr. Adult growth, aging, and the single-tooth implant. Int J Oral Maxillofac Implants. 2000; 15:252-260.
- Agarwal N, Kumar D, Anand A, Bahetwar SK. Dental implants in children: A multidisciplinary perspective for long-term success. Natl J Maxillofac Surg. 2016; 7:122-126.


Add comment