
Torque tells part of the story – ISQ reveals the whole picture
Feb 27, 2026
When assessing implant stability, two metrics dominate the discussion: insertion torque and Implant Stability Quotient (ISQ).
This article draws on selected scientific studies of insertion torque and ISQ to clarify what each measurement represents and how they differ in clinical relevance. Torque provides a single mechanical value at placement, reflecting the rotational friction encountered during implant insertion. While this measurement is useful and routinely documented, it is captured only once and cannot be repeated during healing, which limits its ability to track biological progress.
ISQ, on the other hand, offers an objective and repeatable measurement of lateral stability, enabling clinicians to follow changes in implant stability throughout the healing period. Because torque and ISQ assess fundamentally different aspects of implant stability, understanding how they complement one another supports more confident decision making, particularly when determining the appropriate timing for loading.
Torque and ISQ: Two perspectives
Torque reflects the rotational friction encountered during implant insertion, influenced by factors such as bone density, implant design, and osteotomy preparation. It is recorded as a single mechanical value at placement – even when modern motors display a torque curve, the measurement remains intraoperative and non‑repeatable, providing no insight into the healing process over time.
ISQ, in contrast, measures the lateral stability of the bone-implant interface using resonance frequency analysis (RFA). Unlike torque, ISQ values are repeatable and dynamic. They correlate with micromotion resistance and the progress of implant osseointegration throughout healing. Tracking these changes over time offers a dependable foundation for determining when an implant is sufficiently stable to be safely loaded.
What research shows
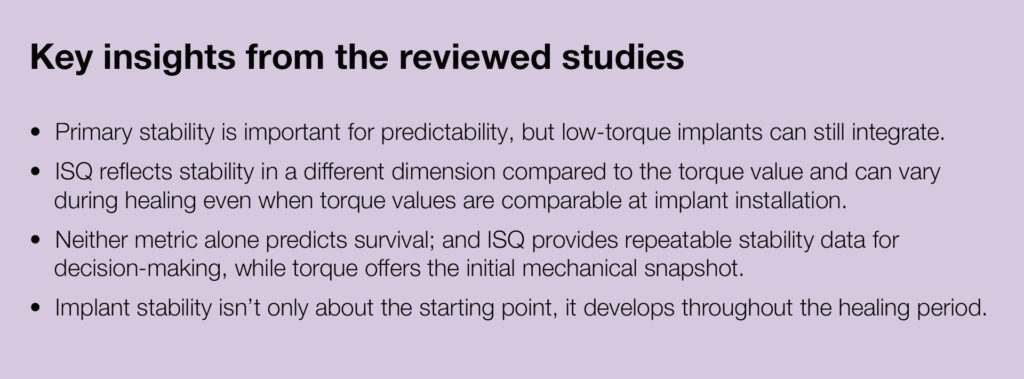
- Primary stability sets the stage, but it’s not the whole story
In several animal studies, it is demonstrated that implants without primary stability fail to osseointegrate, while stable implants achieved up to 81% bone-to-implant contact after nine months [1]. However, clinical data from over 2,600 implants reveal a more nuanced picture: even mobile implants (low torque) integrated successfully in 93.8% of cases, compared to 97.5% for immobile implants. This means torque is useful, yet not the ultimate predictor [2]. - ISQ tracks healing when torque can’t
Research shows that ISQ provides insights beyond what torque alone can offer: it reflects healing dynamics and even implant design. In a canine model, tapered implants had significantly higher ISQ values at placement than straight implants, despite similar torque, highlighting that ISQ responds to design and biological factors [3]. Another clinical study found large torque differences (33.3 ± 13.4 Ncm vs. 17.1 ± 11.2 Ncm) between implants placed in preserved ridges versus pristine bone, yet ISQ values after 10 weeks were almost identical (80.7 vs. 76.4) [4]. - Neither torque nor ISQ alone predicts survival
A systematic review of 37 studies found that although primary and secondary stability are related, neither insertion torque nor ISQ alone predicts implant survival. Notably, very high torque has been associated with an increased risk of marginal bone loss [5]. Together, torque and ISQ offer complementary information, mechanical and biological, and using them together improves predictability and reduces complications.
Clinical interpretation
The findings from the reviewed studies point to a clear conclusion: mechanical and biological stability are two sides of the same coin. Torque gives a mechanical snapshot at placement, while ISQ provides a repeatable way to monitor biological integration during healing, critical for deciding when to load. For clinicians, this means ISQ provides actionable insights for timing loading decisions, turning stability assessment into a continuous process rather than a one-time check.
Further reading
- Lioubavina-Hack, N., N. P. Lang and T. Karring (2006). “Significance of primary stability for osseointegration of dental implants.” Clin Oral Implants Res 17(3): 244-250.
- Orenstein, I. H., D. P. Tarnow, H. F. Morris and S. Ochi (1998). “Factors affecting implant mobility at placement and integration of mobile implants at uncovering.” J Periodontol 69(12): 1404-1412.
- Ellis, R., S. Chen, H. Davies, W. Fitzgerald, J. Xu and I. Darby (2020). “Primary stability and healing outcomes of apically tapered and straight implants placed into fresh extraction sockets. A pre-clinical in vivo study.” Clin Oral Implants Res 31(8): 705-714.
- Ko, Y. C., K. T. Koo, L. Li, D. Lee, Y. M. Lee, Y. J. Seol, T. H. Kim and J. Lee (2025). “Clinical evaluation of implants placed within or beyond the boundaries of the alveolar ridge preservation: a retrospective case series with 10 weeks of observations in 28 patients.” J Periodontal Implant Sci 55(1): 50-61.
- Monje, A., A. Ravida, H. L. Wang, J. A. Helms and J. B. Brunski (2019). “Relationship Between Primary/Mechanical and Secondary/Biological Implant Stability.” Int J Oral Maxillofac Implants 34: s7-s23.


Add comment