Simultaneous Sinus Lift, Bone Augmentation and Implant Placement in the Posterior Maxilla
Clinical case by Dr. Jakob Zwaan D.D.S.
A 62 years old male, that showed good healing after previous implant surgery. An old bridge was present from 14 to 17. 14 had severe periodontal infection, 15 and 16 were already missing.
Author
Dr Jakob Zwaan D.D.S. Private practice, Calusco d’Adda, Italy
Patient
A 62 years old male, that showed good healing after previous implant surgery. An old bridge was present from 14 to 17. 14 had severe periodontal infection, 15 and 16 were already missing. The second molar was, considering it sustained just by itself a 4 element bridge, in good health.
Treatment planning
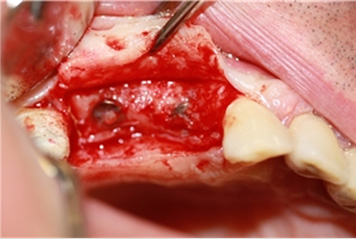
The premolar was extracted and the same bridge used as a temporary solution. Six weeks wound healing guaranteed lower infection risk and easy flap closure during surgery in which 2 implants were placed doing a sinus lift in postion 16 and bone augmentation of alveolar defect related to site 14 (Figures 1-2).
Components Neoss ProActive implants, diameter 4 mm, length 11mm in position 16 and 15mm in position 14. Osteobiol mp3 Tecnoss granules 600-1000 micron. GABA Paroguide resorbable membrane.

Figure 1: Surgical view
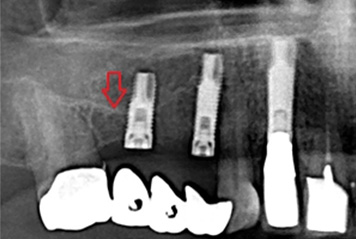
Figure 2: From OPG
Problem
The bone height in position 16 was only 4-5mm. The 14 implant “leaned” on the mesial and palatal bone, but was further exposed for over half it’s length. Insertion torque ranged from 20-25Ncm (16) and 25-30Ncm (14). ISQ values of 52/48 were measured for 16 and of 61/62 for the 14 implant. Encountering low primary stability an instrument was needed to decide when and how to load following reopening surgery after the resorption time of bone substitute as indicated by the producer (5 months).
Solution
During 2nd stage surgery the newly formed coverage of the 14 implant had a “bony” aspect and had a hard consistence, as had the buccal wall of 16 on probing (Fig. 3). The x-ray show newly formed radiopaque material (Fig. 4). ISQ had dramatically increased up to 72 for both implants (Fig. 5), which comforted us enough to proceed immediately with impression taking for the definitive gold-ceramic bridge, which will be screw retained to have the possibility of monitoring implant stability by means of RFA after loading (Figs. 6-10).

Figure 3: Second surgery
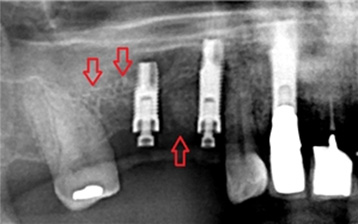
Figure 4: From OPG
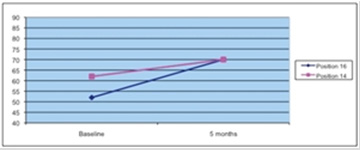
Figure 5: ISQ data
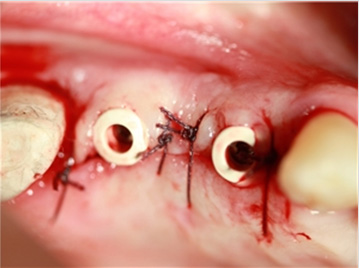
Figure 6: Peek abutments

Figure 7: Soft tissue healing

Figure 8: Papillas formed

Figure 9: Bridge

Figure 10: Radiographs
Sign up to our newsletter to receive more videos and clinical cases like this
